CBpromise
Our promise to you:
Guaranteed product quality, expert customer support.
 24x7 CUSTOMER SERVICE
24x7 CUSTOMER SERVICE
 CONTACT US TO ORDER
CONTACT US TO ORDER
Our promise to you:
Guaranteed product quality, expert customer support.
24x7 CUSTOMER SERVICE
CONTACT US TO ORDER
Cyclic nucleotide phosphodiesterases (PDEs) are enzymes that have the unique function of terminating cyclic nucleotide signaling by catalyzing the hydrolysis of cAMP and GMP. They are critical regulators of the intracellular concentrations of cAMP and cGMP as well as of their signaling pathways and downstream biological effects. PDEs have been exploited pharmacologically for more than half a century, and some of the most successful drugs worldwide today affect PDE function. Recently, mutations in PDE genes have been identified as causative of certain human genetic diseases; even more recently, functional variants of PDE genes have been suggested to play a potential role in predisposition to tumors and/or cancer, especially in cAMP-sensitive tissues. Mouse models have been developed that point to wide developmental effects of PDEs from heart function to reproduction, to tumors, and beyond.
Overview of the PDEs
PDEs, which were identified almost immediately after the discovery of cAMP, represent a large family of ubiquitously expressed hydrolases that control the intracellular levels of cyclic nucleotides by hydrolyzing cAMP and cGMP to 5’AMP and 5’GMP, respectively. Because they catalyze the sole known enzymatic reaction for terminating cyclic nucleotide signals, PDEs are critical regulators of the myriad physiological and pathophysiological processes under cyclic nucleotide control in health and disease.
• Structural organization of the PDEs
The 11 structurally related but functionally distinct gene families (PDE1 to PDE11) that comprise the PDE superfamily differ in their cellular functions, primary structures, affinities for cAMP and cGMP, catalytic properties and responses to specific activators, inhibitors and effectors, as well as in their mechanisms of regulation. Most families contain several PDE genes (for example, PDE1A, PDE1B and PDE1C), which together generate close to 100 PDE isozymes by alternative mRNA splicing or transcriptional processing.
As modular proteins, PDEs exhibit a common structural organization, with divergent amino‑terminal regulatory regions and a conserved carboxy‑terminal catalytic core. Some PDEs specifically hydrolyse cAMP (PDE4, PDE7 and PDE8), whereas others specifically hydrolyse cGMP (PDE5, PDE6 and PDE9), and some hydrolyse (PDE1, PDE2, PDE3, PDE10 and PDE11). The N‑terminal regulatory regions of PDEs contain structural determinants that target individual PDEs to different subcellular locations and signalosomes, and also allow individual PDEs to specifically respond to different posttranslational modifications, regulatory molecules and signals. These structural elements include dimerization domains, autoinhibitory modules, binding sites for ligands and allosteric effectors, phosphorylation sites and other covalent modification sites, domains for isoform-specific protein–protein interactions with specific scaffolds and regulatory partners, and so on (Figure 1).
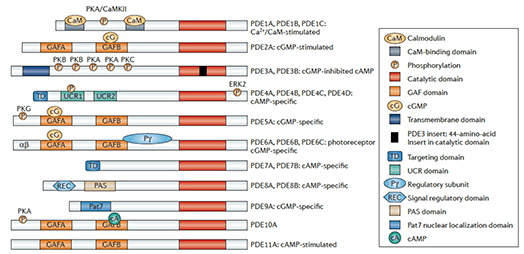
Figure 1. Structure and domain organization of 11 mammalian PDE families
• cAMP and cGMP signaling pathways
Signaling via cyclic nucleotide pathways is central to the function of numerous biological systems. cAMP is typically produced by hormonal stimulation of seven-transmembrane G protein-coupled receptors (GPCRs). Ligand binding to the appropriate GPCR activates the Gs α-subunit of the G protein complex, which exchanges GDP for GTP and is subsequently released from the complex. The activated Gs α-subunit stimulates membrane-associated adenylyl cyclases to convert ATP into cAMP, which in turn activates protein kinase A (PKA), EPAC, or cyclic nucleotide-gated channels (CNGCs). This signaling is terminated when cAMP is degraded by one of the PDE enzymes (Figure 2).
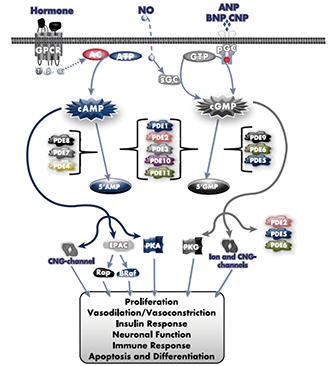
Figure 2. Cyclic nucleotide signaling and regulation.
Phosphodiesterase inhibitors
After the discovery that theophylline, a naturally occurring methylxanthine, inhibits PDEs, thousands of PDE inhibitors (a small number of which are listed in Table 1) have been synthesized, with the aim of improving potency and specificity for inhibition of the various PDEs, not only for research purposes but also for treatment of diseases. All known PDE inhibitors contain one or more rings that mimic the purine ring in cyclic nucleotide substrates of PDEs and directly compete with cyclic nucleotides for access to the catalytic site. The early inhibitors, theophylline and IBMX, are designated as nonspecific PDE inhibitors because they inhibit virtually all PDEs, except PDE8 and PDE9.
| Gene Family | Inhibitor | Use in Clinical Trials |
| PDE1 | Vinpocetine | Anti-inflammatory agent, vasodilator, nootropic for the improvement of memory, urge incontinence, low compliance bladder, acute ischemic stroke |
| PDE2 | PF‑05180999 | Migraine |
| PDE3 | Olprinone | Gastric im acidosis, systemic inflammation after cardiopulmonary bypass |
| Milrinone, cilostamide, amrinone, enoximone | Valvular disease, pulmonary hypertension, cardiac surgery | |
| Cilostazol, K-134 | Cerebrovascular disorders, peripheral vascular disease, intermittent claudication, prevention of stroke, peripheral arterial disease, diabetes mellitus | |
| PDE4 | Ibudilast | Bronchodilator, vasodilator, neuroprotective effects, asthma, stroke, inhibits platelet aggregation |
| Cilomilast | Emphysema, bronchitis | |
| Mesembrine | Anticonvulsant activity, antidepressant, mental illnesses, specifically epilepsy, depression, age-related dementia, and debilitative mental disorders | |
| Etazolate | Alzheimer’s | |
| Rolipram | Multiple sclerosis, MDD | |
| Roflumilast | Chronic obstructive pulmonary disease, asthma | |
| PDE5 | Sildenafil | Pulmonary hypertension, diabetes mellitus, endothelial dysfunction, ischemic stroke, schizophrenia, active digital ulcers, erectile dysfunction, gastroparesis, sickle cell anemia |
| Tadalafil | Benign prostatic hyperplasia, erectile dysfunction, pulmonary hypertension, prostate cancer | |
| Vardenafil, lodenafil, avanafil | Erectile dysfunction | |
| Dipyridamole | Erectile dysfunction, ischemia-reperfusion injury, atherosclerosis, stroke, breast cancer, rheumatoid arthritis | |
| Udenafil | Erectile dysfunction, chronic obstructive pulmonary disease |
Currently, the PDE3 inhibitor cilostazol (Pletal) is widely used to treat intermittent claudication, a peripheral vascular disease; and milrinone (Primacor) is used for acute therapy in refractory heart failure and to stabilize and maintain patients preparing for heart transplants. The PDE4 inhibitor roflumilast (Daliresp) has recently received FDA approval for its use in COPD. The enormously successful PDE5 inhibitors are currently used worldwide for clinical treatment of erectile dysfunction and pulmonary hypertension. Related compounds target other PDEs and show therapeutic promise for a number of disorders.
Conclusions and perspectives
By hydrolyzing cAMP and/or cGMP, PDEs play a critical role in the regulation of cellular functions. Their subcellular localization, structural diversity, and unique regulation allow each PDE variant to regulate compartmentalized cyclic nucleotide signaling pathways and to define specific cell responses in an integrated manner. The intracellular signaling pathways controlled by PDEs can be altered in many pathological conditions, including cancer, inflammatory diseases, neurodegenerative and endocrine disorders, and reciprocally, various pathologies are able to selectively alter PDE regulation, providing a rationale for the use of PDE inhibitors in the treatment of different diseases.
References:
Copyright © Creative Biogene. All rights reserved.