
Several members of the Coronaviridae family continue to spread through the population and usually cause mild respiratory diseases. In contrast, severe acute respiratory syndrome coronavirus (SARS-CoV) and Middle East respiratory syndrome coronavirus (MERS-CoV) are transmitted from animals to humans and cause severe respiratory diseases SARS and MERS in patients, respectively. SARS appeared in Guangdong, China in 2002, and subsequently spread globally, causing 8096 cases and 774 deaths. Intermediate hosts such as civets promote transmission in humans. Currently, there are no antiviral drugs or approved vaccines to treat SARS, and the SARS epidemic of 2002-2003 was finally stopped through routine control measures, including travel restrictions and patient isolation.
In December 2019 a new infectious respiratory disease emerged in Wuhan, China. Subsequently, human-to-human transmission occurred and the disease, now termed coronavirus disease 19 (COVID-19) rapidly spread within China. A novel coronavirus, SARS-CoV-2, which is closely related to SARS-CoV, was found in patients and is considered to be the etiologic agent of the new lung disease. On March 4, 2020, a total of 80,566 cases have been diagnosed in China, with a total of 3015 deaths; a total of 12,980 cases have been confirmed abroad, with a total of 264 deaths.
The spike (S) protein of coronavirus helps the virus enter target cells. Cell entry depends on the binding of the surface subunit S1 of the S protein to cellular receptors, and this binding helps the virus to attach to the surface of the target cell. In addition, entry requires S protein priming by cellular proteases, which entails S protein cleavage at the S1/S2 and the S2’ site and allows fusion of viral and cellular membranes, a process driven by the S2 subunit. The SARS-CoV S protein uses angiotensin-converting enzyme 2 (ACE2) as the entry receptor, and uses the cellular serine protease TMPRSS2 to activate the S protein. The SARS-S/ACE2 interface has been elucidated at the atomic level, and the utilization efficiency of ACE2 has been found to be an important determinant of the SARS-CoV transmissibility. The SARS-CoV S protein and SARS-CoV-2 S protein have approximately 76% sequence identity. However, it is still unclear whether SARS-CoV-2 S protein uses ACE2 and TMPRSS2 to enter host cells like SARS-CoV S protein.
In a new study, German researchers provided evidence that SARS-CoV-2 entry into host cells is dependent on the SARS-CoV receptor ACE2 and it can be blocked by a clinically-proven inhibitor of the cellular serine protease TMPRSS2. In addition, this study also found that antibody responses raised against SARS-CoV can at least partially protect against SARS-CoV-2 infection. These results have important implications for understanding the spread and pathogenesis of SARS-CoV-2, and reveal targets for therapeutic intervention. The relevant research results were published online in the journal of Cell in the form of a manuscript. The title of the paper was "SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically-proven protease inhibitor".
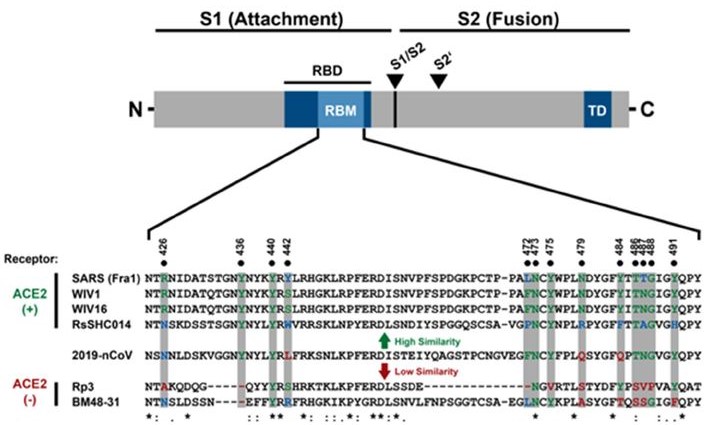
SARS-CoV-2 possesses crucial amino acid residues for ACE2 binding. (Markus Hoffmann et al. Cell, 2020)
The discovery that SARS-CoV-2 uses S protein and ACE2 to enter host cells has also been reported by Zhou and colleagues, suggesting that this coronavirus targets a range of cells like SARS-CoV. In the lungs, SARS-CoV mainly infects lung cells and macrophages. However, the expression of ACE2 was not limited to the lungs, but extra-pulmonary spread of SARS-CoV in ACE2 + tissue was also observed. The same can be expected for SARS-CoV-2, although affinity of SARS-CoV S and SARS-CoV-2 S proteins to ACE2 need to be compared.
In some people's opinion, the moderate expression of ACE2 in the upper respiratory tract may limit the spread of SARS-CoV. Given the potential increase in SARS-CoV-2 relative to SARS-CoV, one might speculate that the new coronavirus may more efficiently use cell adhesion promoters to ensure that a strong infection is established in ACE2 + cells in the upper respiratory tract. This may include binding to cellular glycans, which is a function of the S1 subunit of certain coronaviruses. Finally, it should be noted that ACE2 expression protects the lungs from damage and is down-regulated by the SARS-CoV S protein, which may contribute to respiratory disease SARS. Therefore, it would be interesting to determine if SARS-CoV-2 also interferes with ACE2 expression.
The activation of the coronavirus S protein by host cell proteases is essential for the virus to enter the cell, and this activation involves cleavage at the S1/S2 and S2 'sites of the S protein. The S1/S2 cleavage site of the SARS-CoV-2 S protein contains several arginine residues (multibasic) and has a high cleavage capacity. In fact, the SARS-CoV-2 S protein is efficiently cleaved in cells, and the cleaved S protein can be integrated into VSV virus particles. It is worth noting that this cleavage site sequence can determine the zoonotic potential of coronavirus, and the coronavirus RaTG13, which has the closest relationship with SARS-CoV-2, does not have a cleavage site containing an arginine residue. Therefore, it would be interesting to determine whether SARS-CoV-2 requires a cleavage site containing arginine residues into human cells and how to obtain this cleavage site.
New research shows that the transmission of SARS-CoV-2 also depends on TMPRSS2 activity. In addition, camostat mesylate, which blocks TMPRSS2 activity, inhibits but does not eliminate SARS-CoV-S2 infection of Calu-3 cells. This may reflect the activation effect of CatB/L on the residual S protein. One could speculate that, as reported for MERS-CoV, furin-mediated cleavage of the S1/S2 site in infected cells may promote the subsequent entry of TMPRSS2-dependent target cells. Overall, TMPRSS2 is a host cytokine that is essential for the transmission of several clinically relevant viruses, including influenza A virus and coronavirus. TMPRSS2 is essential for development and homeostasis and therefore constitutes an attractive drug target. It is worth noting that the serine protease inhibitor carmustine mesylate that blocks TMPRSS2 activity has been approved for use in humans in Japan, although its indications are not related to SARS-CoV-2. Therefore, this compound or related ones with potentially increased antiviral activity could be considered for off-label treatment of SARS-CoV-2 infected patients.
In conclusion, this study provides crucial new insights into the first step of SARS-CoV-2 infection — the entry of virus into cells — and the identification of potential targets for antiviral intervention.
References
- Markus Hoffmann et al. SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically-proven protease inhibitor. Cell, 2020
- Zhou P, et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature, 2020: 1-4.